

You have gone to see a doctor and you were told you have a herniated disc. What does that mean? Sometimes medical jargon like “herniated disc” needs to be explained in a less threatening way. In this article I will be talking about the anatomy of a herniated disc, I will be discussing advanced imaging such as MRI and CT scans, I will be touching on treatment options that help get rid of the pain and limitations associated with a herniated disc, and finally what you can do to help yourself.
What it is?
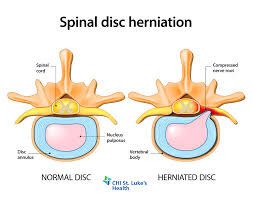
A herniated disc needs to be explained by discussing what a normal intervertebral disc is in our spines. A disc in your spine is a structure that is mainly made of fibrocartilage that acts to help dampen force and also provide stability, movement, and strength to the spine. The disc is located between the bones of the back, we have a total of 23 discs in the human spine. The disc itself is composed of an inner portion called the Nucleus Pulposus, an outer portion called the Anulus Fibrosis, and an attachment site called the Vertebral End Plates.

A disc herniation is defined as a localized displacement of disc material beyond the limits of the IVD space. Where a disc herniation becomes problematic is when it starts to affect the spinal nerve root that is close by.
When the nerve root is effected a patient can experience back pain, Weakness in the leg and/or foot, or tingling (a \”pins-and-needles\” sensation) or numbness in the leg and/or foot. We term these symptoms sciatica.
Good News
When you are dealing with a herniated disc, you probably just want to know how long it is going to take to get better. The research says that if you stay active, your back pain and/or leg pain will get better. Did you know that a herniated disc can be reabsorbed by your body?! One particular research study looked at 160 patients who had a herniated disc on MRI. They were looking at the factors that would predict a better ability of the disc to be naturally reabsorbed. They re-scanned 73 of those patients at 2 months, and 55 of those patients at 12 months. What they found was that there was significant reabsorption of the disc material at 2 months which continued up until 12 months post initial MRI scan.1 This study looked at finding prognostic factors that are related to a patient having a higher reabsorption rate. They found that if you were 41-50 years of age, had a certain degree of disc herniation (measured by the Kamori Classification system) and also higher degrees of rim thickness as seen on MRI you would have a higher chance of reabsorption. The main takeaway is that discs reabsorb and heal!
Treatment Options
The next logical question you may be asking when dealing with a herniated disc is, “What are my options for treatment?” The most typical course of herniated disk treatment includes a visit to your primary care physician and a prescription for medication. These may include anti-inflammatories, steroids, or even muscle relaxers. Physical therapy is a conservative option that can improve function, reduce pain, and treat the impairments that are keeping you from doing the things you love. Other options include getting an injection or having surgery. These are obviously the most invasive of the options. So how do you know which one is right for you.
Let me share some research studies that compare these interventions. The first study compared surgery to conservative care. This study included 283 patients who had severe sciatica. Of the patients, 89% randomised to early surgery underwent microdiscectomy after a mean of 2 weeks, while 39% of patients randomised to conservative treatment underwent surgery after a mean of 19 weeks.2 Relief of leg pain was faster for patients assigned to early surgery. Intention-to-treat analysis showed statistically significant more leg pain relief in favour of early surgery as compared with prolonged conservative care at 3 months. The median time to recovery was 4.0 weeks for early surgery and 12.1 weeks for prolonged conservative treatment. At 1 year of follow-up, however, 95% of patients in both treatment groups had experienced satisfactory recovery, and no subsequent differences were found.
What do all these fun facts mean? If you can just wait it out and get with a clinician who provides the most cutting edge techniques, you can get a great outcome and you can AVOID SURGERY! The subgroup of 55 patients with persistent sciatica and conservative treatment followed by surgery had a similar improvement in these scores at 1 year as compared with patients allocated to early surgery. As long as the patients were not having any red flag symptoms which include continued weakness in a leg or foot, numbness in groin or the buttocks, difficulty walking, standing, or moving, loss of bowel or bladder control, fever, unexplained weight loss, or other signs of illness. This goes to show that even if you attempt conservative care and decide that you want surgery, your outcomes will be the same as the people who had elected to have surgery early on. I would rather try to avoid surgery at all costs and try to let my body naturally heal.
What can you do to help yourself?
Just like anything in life, not all things are created equal. When choosing a physical therapist to help with your herniated disc or sciatica you want to find one that knows the McKenzie method and uses a particular treatment approach. Find out more information about the McKenzie approach here. This treatment approach is called the test/retest approach. Your skilled physical therapist should first take a thorough history. This is where my first bit of advice comes in. Try to be very specific with things that make your symptoms worse and things that make it better. This may be a movement, a position, a stretch etc. Often when treating patients with a herniated disc, there is something that makes your symptoms change. Also the patterning of your symptoms throughout the day is important for the therapist to know. Is your pain worse in the morning? Does it get better as the day goes on? Equipped with this information from you, your therapist can better diagnose how best to help you.
One research study that looked at utilizing the McKenzie treatment approach involved 180 patients with sciatica who were randomized into two groups. One group got treatment over an 8 week period (average was just 5 visits) in the McKenzie Method and the other group performed cardiovascular exercise. The patients in the McKenzie group improved in most clinical outcomes including pain, functional status, and clinical findings. Perhaps most telling is that the number of patients in the cardiovascular exercise group electing surgery within one year was five times greater than that with the McKenzie Method group.3
I (Dr. Murphy) am trained in the McKenzie method and am the owner at Pinnacle Physical Therapy. We are located at 5507 Ranch Dr Suite 203 in West Little Rock, Ar. We offer a free discovery visit. We would love to set up a time to chat with you in person or over the phone to listen to your story and see if we feel we can help you solve your problem. You can text or call 501-529-2010 to set up your discovery visit.
We look forward to helping you reach your Pinnacle!
Dr. Brian Murphy
*The information in this article is broad information and is not meant to create a patient clinician relationship with Dr. Murphy. It is always advised that you see your physician before starting any exercise program. The best way to receive care for your particular situation is to get an appointment for a thorough assessment by a trained medical professional.
References
- Autio RA, Karppinen J, Niinimäki J, et al. Determinants of Spontaneous Resorption of Intervertebral Disc Herniations. Spine. 2006;31(11):1247-1252. doi:10.1097/01.brs.0000217681.83524.4a.
- Peul WC, van Houwelingen HC, van den Hout WB, Brand R, Eekhof JA, Tans JT, Thomeer RT, Koes BW (2007) Surgery versus prolonged conservative treatment for sciatica. N Engl J Med 356:2245–2256
- Reference: Nordin M, Belague F. Exercise may be beneficial for patients with chronic, severe sciatica who would normally qualify for surgery. Evid Based Med. 2013; 18 (2): 63-64.